

Introduction
Coronavirus disease (COVID-19) may induce a hypercoagulable state, leading to microvascular and macrovascular thromboses, as shown in observational and autopsy studies (Giannis, Ziogas, and Gianni 2020; Carsana et al. 2020; Lax et al. 2020). Empiric therapeutic anticoagulation has been recommended by some authors (Barnes etal. 2020; Kollias et al. 2020). The risks and benefits of empiric therapeutic anticoagulation in COVID-19 is unclear and subject to further investigation. The objective of our observational study was to determine if there was a survival benefit with the empiric use of therapeutic anticoagulation in hospitalized patients with COVID-19 compared to prophylactic doses of anticoagulation.
Materials and methods
We performed a retrospective, multi-institutional cohort study of patients over the age of 18, admitted to hospital with COVID-19, between March 10, 2020, and May 3, 2020. We excluded patients who were discharged or died on the same or following day of hospital admission. Our 'exposed' group was defined as any patient who received therapeutic anticoagulation during the hospitalization, with low molecular weight heparin (LMWH), unfractionated heparin (UFH), direct-acting oral anticoagulants (DOAC) or warfarin. Our 'control' group consisted of patients who received a prophylactic dose of anticoagulation during their hospital stay.
The primary endpoint was the time from admission to discharge or death. Patients without a primary endpoint event had their data censored on May 20, 2020. Cox proportional-hazards regression models were used to estimate the association between treatment and in-hospital mortality by adjusting for demographic and clinical factors. Before conducting the outcome analyses, multiple imputations (10 imputations) were performed for missing data. Due to the non-randomized nature of the study and the reduction of the effects of confounding, inverse probability weighting was utilized. Secondary objectives included requirement for intubation, duration of intubation, length of hospital stay, and readmission rates.
Results
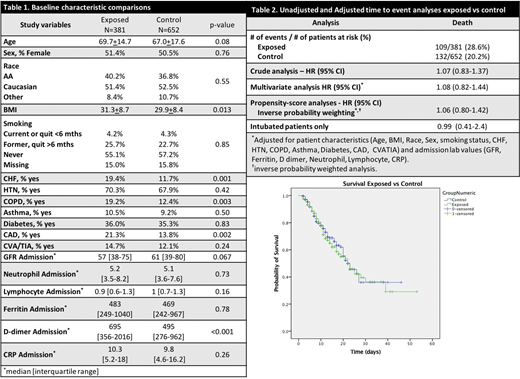
A total of 1033 patients were included in the study. Among them, 381 patients (36.8%) received therapeutic doses of anticoagulation with UFH, LMWH, warfarin, or DOAC. The remaining 652 patients (63.1%) received prophylactic doses of anticoagulation. Baseline characteristics showed that the group with therapeutic anticoagulation had higher body mass index, higher rates of congestive heart failure, chronic obstructive pulmonary disease, coronary artery disease, and admission d-dimer levels (Table 1) and significantly higher mortality rate (28.6% vs. 20.2%; p=0.002) (Figure 1, survival curve). However, there was no difference in the risk of in-hospital mortality between the groups using unadjusted and adjusted Cox regressions (Table 2). No benefit was seen in the subgroup analysis of intubated patients as well. In addition, the exposed group had higher rates of intubation (13.3 % versus 7.7%; p = 0.01) and were more likely to be re-admitted (10.3% versus 5.2 %; p = 0.007; survivors only). Median length of stay was significantly longer in the exposed group (7 vs. 6 days; p=0.028; survivors only).
Conclusion
Our result showed that therapeutic anticoagulation in hospitalized COVID19 patients was not associated with a reduction in in-hospital mortality compared to prophylactic anticoagulation. In addition, patients in the fully anticoagulated group were intubated more often, had a longer length of stay, and higher readmission rate. Well-designed prospective randomized studies are needed to define the dose of anticoagulation in COVID 19 patients.
Limitation
Retrospective cohort design, as well as multi-institutional nature.
No relevant conflicts of interest to declare.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal